(Thinking that Reading, Writing and Arithmetic are the three R’s doesn’t seem to me to represent a high degree of literacy!)
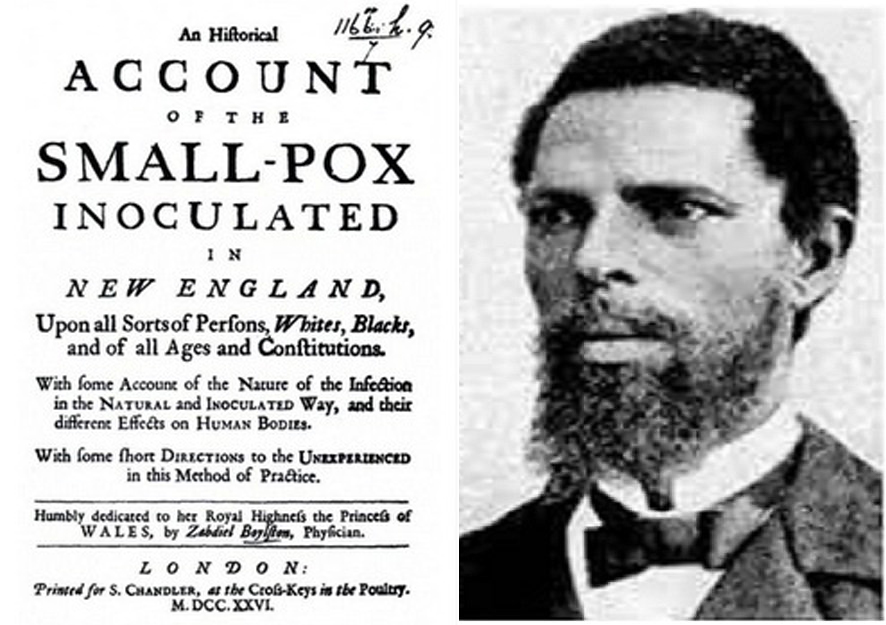
Back in March, I noted that three hundred years ago, a fatality rate of 2.5% from smallpox infection after variolation was considered an acceptable risk to prevent a far deadlier death toll up to 10 times greater from the disease itself. Today, countries are suspending vast inoculation drives on the basis of risks of the order of parts in a million. There are reports of rare blood clots arising in recipients of both the AstraZeneca and Jannsen vaccinations and in February, there were also reports of cases linked with the Moderna and Pfizer vaccines.
This news has had conflicting effects on me, depending on whether what I feel about them dominates what I think, or, to put it another way, whether I can set aside my System One reaction and indulge in System Two reflection. In that vein, I want to examine System One and System Two approaches to the Risk Reward Ratio.
In my post ‘Skin in the Game’, I mentioned a message in my local chat group about a 42-year-old female nurse at a hospital in Greece whom it was reported had symptoms of a rare autoimmune condition called Guillain-Barré Syndrome (‘GBS’) immediately after receiving a second vaccination against Covid-19. This short 29 word message concealed so much beneath the surface that I promised at some point to dig deeper. Now is the time!
Much can be gleaned about our attitudes to vaccination from this episode. The principle questions that posting this message raises seem to be:

- Why was the story interesting to the person who posted it?
- Why did the person posting it feel it was important to share it?
- What was the source of the story?
- Were there consequences attached to the report?
- What ultimately happened to the Greek nurse in the story?
- Was it GBS and what is GBS anyway?
- What is the probability of suffering from GBS in the general population?
- How does that relate to vaccination associated risks?
Why was the story interesting to the person who posted it?
Of course, only that person can answer the question. However, it seems entirely possible to me that, in the context of the group, they had found a story which seems to support one of their deeply held beliefs, viz that the vaccine is highly dangerous and has unexpected consequences. And, above all, for those reasons, it should not be taken.
The suspicion of connections between GBS and vaccination dates back to 1976 when a mass vaccination campaign in the USA in response to the fear of a swine flu pandemic led to an increase in reported cases of GBS. Although this was reported as an eightfold increase, later studies calculated that the actual number of additional cases amounted to one additional case of GBS for every 100,000 doses administered.
Why did the person posting it feel it was important to share it?
Presumably, if those were the reasons the story was of interest, the person who posted it wanted to convince others of the dangers of a vaccine, maybe from a genuine wish to prevent them coming to harm, but also possibly as a form of group and personal validation. Sharing such information validates the group and re-enforces our individual sense of justification.
What was the source of the story?
The story originated from a local leader of the trade union representing the health care worker, not from a hospital or government source.
Were there consequences attached to the report?
The union leader announced their intent to sue for damages on behalf of the nurse. The police launched an inquiry into whether he committed the crime of ‘spreading false news’ by expressing with certainty that the woman’s paralysis was a side effect of the vaccine.
What ultimately happened to the nurse in the story?
A subsequent report states that in fact, after vaccination, the nurse ‘had a bit of a fever and felt some numbness in her limbs’. After a period of rest at home, her condition improved.
Was it Guillain-Barré Syndrome and what is Guillain-Barré Syndrome anyway?
The subsequent report suggests this may not have been a case of GBS. Guillain-Barré Syndrome is an autoimmune neurological disorder which can be triggered by a number of stimuli. Most start shortly after a respiratory or gastrointestinal viral infection though occasionally surgery can trigger the syndrome. In rare cases, as with the 1976 swine flu vaccine, vaccinations have been implicated.
What is the probability of suffering from Guillain-Barré Syndrome in the general population?
The overall incidence of Guillain-Barré Syndrome in populations in Europe and North America is estimated to be between 11 and 18 per million people per year.

In this context, this means that if you take a million people, vaccinated or unvaccinated, it is highly likely that over a period of a year, between 11 and 18 of them would show symptoms of GBS, irrespective of their vaccination status. In a population over 50 years of age, the likelihood of GBS is higher, between 17 and 35. This is why when assessing the risks of vaccines in huge numbers of people, scientists take time to compare the risk of extremely rare conditions like GBS amongst vaccinated populations with the incidence amongst unvaccinated population.
How does that relate to vaccination associated risks?
As at today, about 550 million people have received a Covid-19 vaccine world-wide. In all likelihood around 600 of those would have developed GBS over the course of a year in any event, so nothing can be read into individual cases of GBS presenting after vaccination. In particular, many countries have vaccinated older citizens first, in whom the natural incidence of GBS is higher.
However, in a manner with similarities to the incidence of blood clots resulting from Covid-19 compared with the possible risk from some of the current Covid-19 vaccines (see ‘Risk and Reward – Blood Clotting With and Without Vaccination‘), there is clear evidence that the incidence of developing GBS from hospitalisation with influenza infection is around 7.2 cases per million patients hospitalized with influenza compared with 1.6 cases per million vaccinated people following the 2009 H1N1 ‘flu vaccination program, roughly the same as for the seasonal flu vaccine.
In other words, people hospitalised with flu were almost five times more likely to suffer the effects of GBS than those who had been vaccinated, and those who had been vaccinated and developed GBS were within the range of annual naturally occurring GBS from all sources.
Risk Reward Ratio
The Risk Reward Ratio can be well understood in financial terms. The principle is that rewards (in this case financial returns) are proportional to the risks taken. In other words, it’s safer to put your money in a bank than in the stock market, or, riskiest of all, betting on a 40:1 outsider in the Grand National. In a bank in industrialised economies at the moment, you may get returns of the order of less than 1% per year, investing in the London stock market could make you 17% in 2019, but if you back the aptly named ‘Shattered Love’ in the Grand National and it were to romp home at 40:1, your returns are 4,000% in a matter of minutes. As risk increases, if you succeed, your rewards increase. The Risk Reward Ratio is the basis for entrepreneurial activity in capitalist economies.

But this is where System One and System Two thinking about the Risk Reward Ratio part company. The odds of winning the UK national lottery are an astronomical 45,057,474 to one! And in spite of this, 70% of UK citizens over the age of 18 take part in the national lottery on a regular basis. System Two thinking would compute that the likelihood of winning are so low that both your time and money would be better off spent elsewhere. But a complex system of neurotransmitters, such as serotonin, dopamine, endogenous opioids and hormones mean that we get a hit from irrational gambling and allow System One feelings to assert, in the words of the National Lottery advertising campaign, ‘It Could be You’. And I, for one, believe them!
Risk and Reward – Blood Clotting With and Without Vaccination
And exactly the same thinking/feeling polarity seems to dominate our approach to vaccine risk. Although the risks of developing a fatal blood clot from receiving an AstraZeneca vaccine according to the European Medicines Agency seems to be less than one in a million (18 fatalities from 25 million vaccinees), we are all convinced ‘it could be me’.
To put that in perspective, around 1 in 2,000 women each year will develop a blood clot from taking the combined oral contraceptive pill, and 1 in 1,000 people a year will develop a blood clot from air travel. On the other hand, in an echo of the findings about developing GBS after a flu vaccine I cited before, a non-peer reviewed study by a team at Oxford University has deduced that the risk of developing a serious blood clot in the brain is 8 to 10 times higher in people with Covid than those who get a vaccine.
And yet, System One Thinking persists in telling us, ‘It Could Be You’!
Risk of death can be measured in a unit called a ‘micromort’ which is defined as a risk of dying of one in a million. It has been calculated that driving a distance of about 250 miles (400 km) carries a risk of one micromort (I’m not sure that applies to driving in India!). In other words, if you are driving from Tampa to Fort Lauderdale in Florida, or London to Newcastle in the UK, or Berlin to Hamburg in Germany, you are taking a one-in-a-million risk of being the victim of a fatal road accident during the journey. At 1.6 micromorts, the risk associated with GBS arising from a flu vaccination, therefore, is roughly the same as the risk of death when driving 400 miles, or London to Edinburgh.
With that background, we can look afresh at the numbers of fatalities arising from blood clots after receipt of the AstraZeneca vaccine. Taking the UK as a good example because of its high rollout rate of this vaccine and its centralised healthcare and reporting systems, 79 cases of blood clots following the first dose of the vaccine had been reported by the end of March, 19 of which were fatal. By then, over 20 million doses of the AstraZeneca had been given in the UK, so the overall risk of these blood clots after the first dose of the vaccine is approximately 4 in a million and of death from those clots about 1 in a million. Which is one micromort – the same risk as our earlier car trip from London to Newcastle.
As the risk of vaccine associated blood clots seems to be a function of comparative youth and the risk of covid-19 related death a function of comparative elderliness, there is a helpful graphic from Cambridge University to visualise the Risk Reward Ratio:
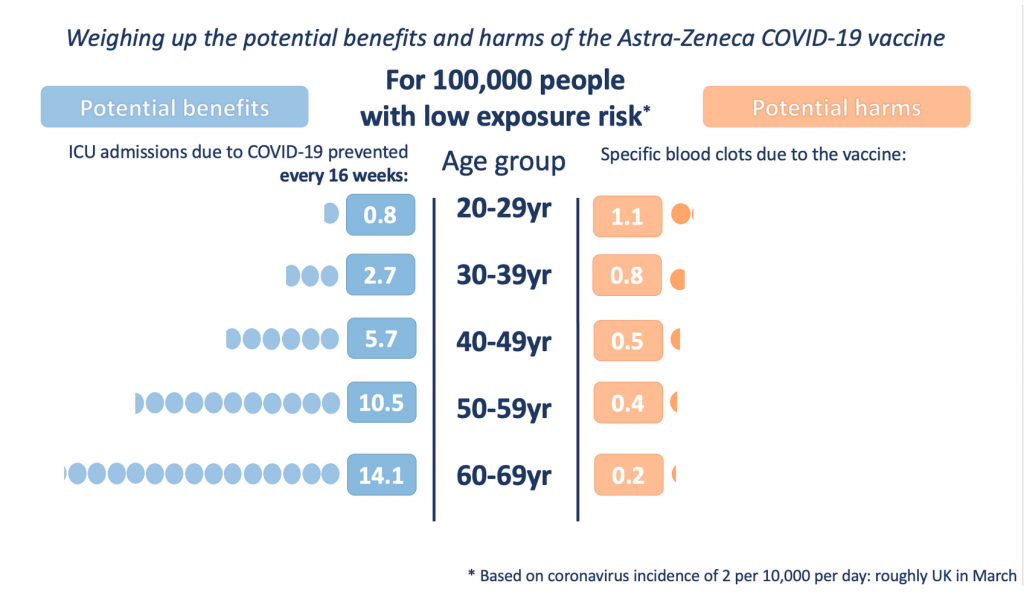
The risk of blood clots from vaccination is shown on the right side, and is never very high, though clearly decreasing with age. On the left, the reward is shown inversely as the risk of severe Covid-19 disease which is reduced by up to 94% a month after the first vaccine dose.
For the 60-69 age range, the risk of severe Covid-19 following infection is almost 30 times greater than the risk of a blood clot following vaccination. But, for someone under the age of 30, the risk reward ratio is almost even, with the risk from clotting slightly higher than from severe Covid-19.
However, there is also the public versus personal health conundrum. As not vaccinating younger people would prevent societies achieving herd immunity (estimated as requiring immunity in 60 to 72% of the population), then from a societal and public health point of view, offering a different vaccine to younger people is crucial, something the UK government has already announced.
Whatever our System One mind might feel, the message from System Two is pretty clear.
So the upshot of all this is that you are hugely more likely to come to harm from Covid-19 than from any of the currently approved anti-Covid vaccines. And it’s not even close!
Meanwhile, Covid-19 has overwhelmed the world’s largest producer of vaccines in a nightmarish Indian Summer….
Thank you again, Gupi, for another sage elucidation of complicated matters. The sad part for me is that no amount of rational understanding or statistical logic makes a dent in the brains of my broad-reaching anti-vaxxer and conspiracy theorist friends. They would cut you off at the roots by simply claiming that all your institutionally sourced figures are bunkum – fake news, fabricated by ‘them’ to lull you into volunteering to turn yourself into zombies. And without your statistics and figures, the whole caboodle amounts to nothing. 😩
Taking two steps away from everything you have so beautifully mapped out for us here, is the Zen understanding that “Not knowing is the most intimate”… The fact that I can no longer have a serious conversation with any of said CT friends (there are four of them close to me here) pushes me to ask myself what is existence trying to teach me in this?
Maybe that’s a question for your blog? I don’t know.
Thanks for the comment.
In ‘Pink Elephants and Little Green Men’ I listed 6 categories of attitude to the pandemic. Your friends appear to be in Category 6 – ‘Distrustful, researched but been misinformed, decided, absolute ‘no’ to vaccines and quite possibly ‘no’ to the existence of a pandemic or even coronaviruses’. They ‘feel’ that they are right. As data have not been part of forming their decision, data cannot be a part of changing their position.
In many ways, I agree with them (!). But for reasons I will explore another time, their model of global elites controlling the world in some cabalistic way seems too improbable. Humans (and probably alien reptiles too) are way too incompetent to be able to do that.
What I do agree with, however, is that some politicians and some business interests (and probably others such as scientists even) have taken the opportunity of a pandemic to enpower, enrich or aggrandise themselves, and that it will take time, motivation and quite probably violence for societies to claim back the imbalances that have been created. In ‘Entering the labyrinth’ I mentioned a view that the English Gunpowder Plot of 1605 was a real plot, but that politicians in the form of James I’s chief minister took control of the course of events using it to suppress the Catholic minority. It took over 200 years to reverse the repressive legislation that followed. As the German philosopher Georg Hegel famously said, ‘The only thing that we learn from history is that we learn nothing from history’….
An interesting article David although the switching of measures of risk through it makes my slothful mind complain.
Even when the data is freely available and the scientists are agreed on the risk reward levels, it’s noticeable that the leaders of many European countries decided to overrule them and put political considerations ahead of the lives of their subjects. Sad too that their citizens chose to believe them over the scientists. It looks like logic and truth are the main victims of this pandemic
Hi Dave
Thanks for the comment. I was aware of the mixing of terms and I have several excuses available, but the main reason is that I came across the unit of a ‘micromort’ during my research for the piece and clearly it was an appropriate unit for my purposes. The other ancillary reasons (excuses) include that a micromort measures risk from a single event such as a vaccine dose, but does not apply well to an annual risk, such as the risk of death from GBS. And I am also aware that the risk of a blood clot from a daily dose of a pill does not compare directly with the risk from a single inoculation. However, my association here was not intended to be mathematical but psychological, pointing out that we willingly engage in behaviour which is statistically equally as dangerous as a vaccination (such as car journey from London to Edinburgh) without a second thought. Yet allowing a stranger to inject an unknown substance into my body evokes a layer of feelings that the car journey does not.
Your other point is about politicians making decisions not based on scientific understanding is more complex. I will explore the role of nationalism in the pandemic to some degree when I look at the pandemic in India in the piece I am in the middle of this week. Clearly politicians make decisions for political reasons. As I suggested in ‘Robin Hood and the Coronavirus’, populations will endure a lot of sacrifice in exchange for security and economic stability. But politicians are in trouble if people perceive that this contract is broken, and the pandemic has put that at risk: decreased safety and prosperity is now combined with increased repression. Donald Trump famously opined that the cure to the pandemic (i.e. lockdown) could cause more damage than the virus. This is based on a theory that reduction in GDP in itself leads to increased mortality rates. Some economists and politicians hold to this and their decisions, which can be characterised as putting citizens’ lives at risk by easing lockdown, are often justified by this. Counter-intuitively, there is much to suggest this theory is flawed.